Coronavirus Update: Sindh’s infection tally surges to 30,000
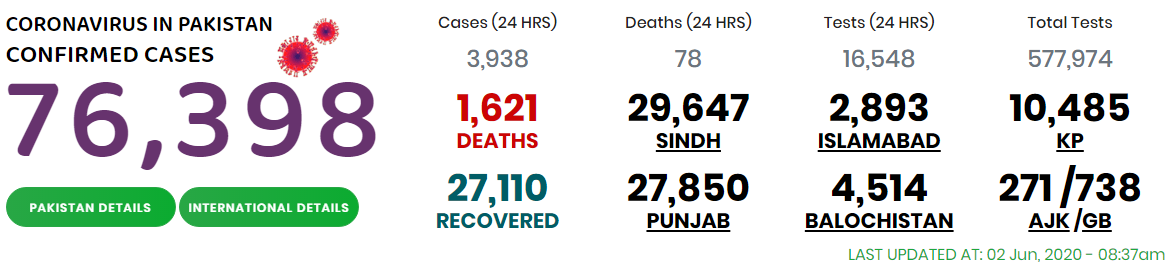
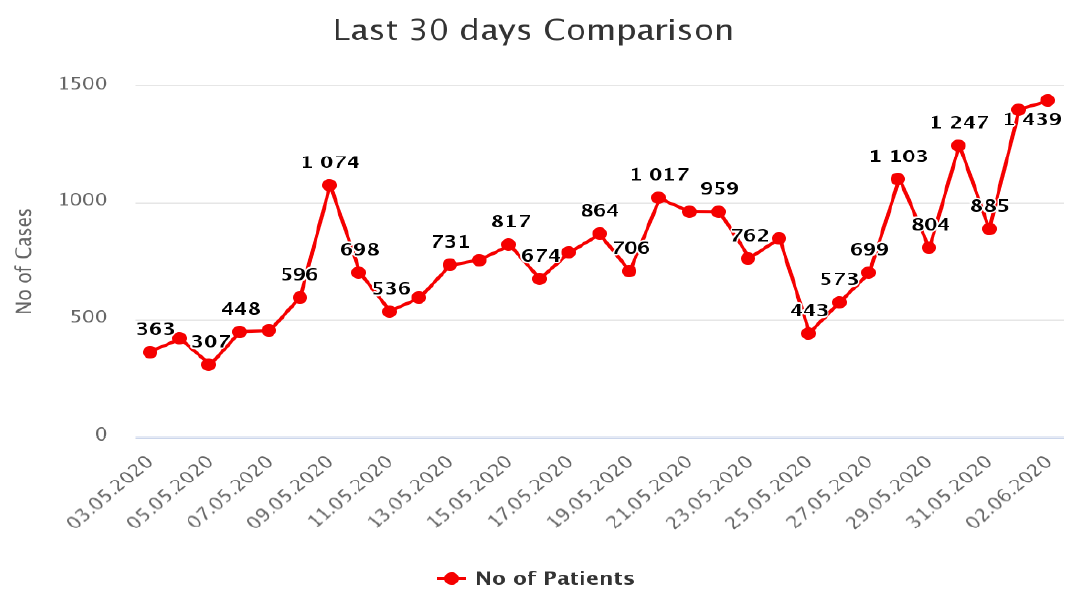
KARACHI: At a time when the government was allowing more and more relaxations in the COVID-19 lockdown, Sindh’s average daily rate of new coronavirus infection jumped to 25.17% for the preceding week on June 2 when its overall infection tally surpassed 30,000 after registration of another 1,439 cases, an all days’ highest, with 23 related fatalities.
A study of the official COVID-19 data of Sindh revealed that the number of new infection rate decreased by four per cent in comparison to the preceding day but was still higher than what was being observed before Eid vacations. Sindh on May 27 witnessed a record daily increase in its COVID-19 positivity rates at 32.10%.
The province’s coronavirus positivity rate on May 21 was at 15.99%, which rose to 23.85 on May 24 and 24.62% on May 26. The number of cases decreased to 22% on May 31 when 885 suspected cases, out of 4,100 samples, tested positive for the virus.
According to an official report, as many as 16 COVID-testing laboratories, operating in the public and private sectors, conducted across the province as many as 5,454 tests during the last 24 hours ending at 9 am on June 2, out of which 1,500 (27.5%) were found positive.
Among the laboratories, JPMC performed four tests and detected all (100%) positive while Indus Hospital centre tested 1,285 samples and found 36% of them positive. Other centres which conducted tests included SIUT (69%), DUHS (50%), Hashmanis (38%), AKUH (36%), CHK (36%), Gambat Institute of Medical Science (35%), Liaquat University of Medical and Health Sciences (15%), and others.
According to a health department summary, a total of 1,149 infections were found at Karachi, followed by Larkana (50), Hyderbaad (47), Sukkur (40), Khairpur (33), Ghotki (27), Shaheed Benazirabad (17), Badin (16), Sanghar (13), Jamshoro (10), Kambar Shadadkot (6), Shikarpur (6), Sujawal (5), Dadu (3), Jacobabad (3), Thatta (2), Kashmore (2), Tando Mohammad Khan (1), Matiari (1) and Umrkot (1). Among the interior districts, Larkana led the list with a cumulative 1,002 cases followed by Hyderabad (977), Larkana (770), Khairpur (703), Ghotki (635) and other districts.
As many as 23 new deaths of COVID-19 were confirmed by the health department on June 2. Karachi reported 17 deaths, 12 men of ages ranging from 42 to 95 years, and five women in the age brackets of 42 to 75 years, while Sanghar, Dadu, Shikarpur, Larkana, Sujawal and Hyderabad reported one death each of men, aged from 40 to 67 years.
According to an official source, as many as 446 COVID-19 patients have lost their lives in public and private hospitals, including AKUH (54) CHK (44), Indus Hospital (45), JPMC (64), DUHS Hospital (67), SIUT (59), Ziauddin (29), PNS Shifa (14), LUMHS Hyderabad (12), GIMS Khairpur (7), GMMMC Sukkur (5), Lyari General Hospital (9), NICVD Karachi (4), OMI Hospital (3), Patel Hospital (3), South City Hospital (4), SMBB Trauma Centre Karachi (4) and others.
In his routine statement, the Sindh Chief Minisiter, Syed Murad Ali Shah, remarked that 953 more patients have recovered from the diseases, while 358 out of 1,098 hospitalized patients were in critical condition.
He urged the people not to take unnecessary advantage of the relaxations allowed in the lockdown and follow the standard operating procedures for their health safety.
A source disclosed that only one out of 367 prisoners found positive for coronavirus at the Central Prison Karachi has recovered from the disease so far.
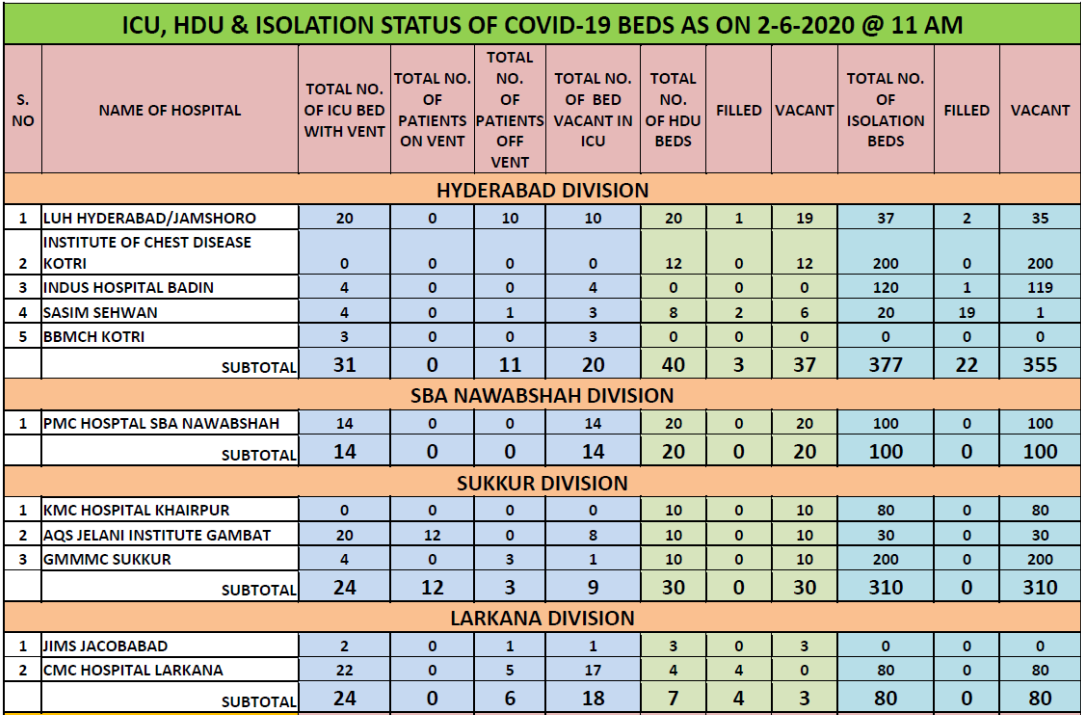
Another source revealed that in all 12 ICU beds in four hospitals, 28 HDU beds at four hospitals and 168 isolations beds at five hospitals were in use as on June 2 morning.
In the meantime, a national position paper has highlighted the potential reasons for risk in critical patients. As per the report, the reasons included the overall rise in number of daily detected cases and new hospital admissions; shifting to policy of admission of moderate to severe patients only; delayed arrival of patients getting critical at homes; differential implementation of the clinical management SOPs; and changing risk perceptions of patients as well as doctors due to increased deaths and media coverage–PNFS